Research Article
Volume 4 Issue 1
Influence of Different Types of Surface Treatment on Adaptation of Ceramic Laminate Veneer
Roweena Alaa El Din1, Shaimaa Ahmed Abo-El Farag2 and Mohamed Hamed Ghazy3*
1Dentist at the ministry of health, Egypt
2Associate professor of Fixed Prosthodontics, Faculty of Dentistry, Mansoura University, Egypt
3Professor & chairman of Fixed Prosthodontics Department, Faculty of Dentistry, Mansoura University, Egypt
*Corresponding Author: Mohamed Hamed Ghazy, Professor & Chairman of
Fixed Prosthodontics Department, Faculty of Dentistry, Mansoura University, Egypt.
Received: February 16, 2020;; Published: February 28, 2020
Abstract
Objectives: This in-vitro study investigated the effect of different surface treatment materials on marginal and internal adaptation of ceramic laminate veneer.
Materials and Methods: Twenty-eight CAD/CAM fiber reinforced composite abutments were prepared to receive zirconia laminate veneers. All veneers were divided into four groups (n=7) based on their surface treatment. Group A: treated with air abrasion only (control group). Group AZ: treated with air abrasion then Z-Prime Plus. Group AB: treated with air abrasion then All-Bond Universal. Group AZB: treated with air abrasion, Z-Prime Plus and then All-Bond Universal. All veneers were cemented to their corresponding abutments using adhesive resin cement. After 24 hours water storage, all specimens were sectioned mesiodistally and incisogingivally. Absolute marginal gap (AMG) at cervical and incisal areas and internal gap (IG) at six different locations were measured under stereo-microscope. One-way ANOVA followed by post hoc Tukey tests were used to test the difference between groups (α= 0.05).
Results: The mean values of AMG of tested groups were 151.07 ± 5.75 µm, 95.93 ± 6.50 µm, 127.50 ± 4.79µm and 107.14 ± 7.42 µm for groups A, AZ, AB and AZB respectively. The mean values of IG of tested groups were 167.62 ± 4.92 µm, 85.95 ± 4.39 µm, 135.48 ± 5.22 µm and 140.48 ± 2.67 µm for groups A, AZ, AB and AZB respectively. These results indicated that AMG and IG were significantly lower in groups AZ, AB and AZB than the control Group A (p<0.001) and Group AZ showed significantly lowest AMG and IG than all other tested groups.
Conclusion: Surface treatment using air abrasion then Z-Prime Plus effectively improved the marginal and internal adaptation of zirconia ceramic laminate veneer.
Introduction
With the development of modern technology, esthetics restorative dentistry has reached a new spectrum. [1] Nowadays, people seek to have whiter teeth to mask the effects of aging that their smile reveals. Masking the discolored teeth with a lighter colored restoration that matches the adjacent natural teeth such as composite resin or porcelain is one of the best treatment options for this problem. [2]
Ceramic veneers are conservative treatment for some cases such as; discolored, slight malpositioned or fractured anterior teeth, diastema, enamel defects and aging.[3] Long term success of ceramic laminate veneers is affected by many factors such as: Bonding properties, mechanical strength, marginal adaptation and internal adaptation. [4]
The retention of ceramic veneers depends totally on bond strength between the ceramic material and the tooth structure. [5] Ceramic surface treatment is necessary to achieve a predictable bond, [6] it varies according to different ceramic materials. For glass based ceramics, the most common method is hydrofluoric acid etching (HF) followed by application of silane coupling agent. [7]
For Zirconia based ceramics (free from silicon dioxide) neither etching with hydrofluoric acid or other acids nor applying silane coupling agents can achieve adequate resin bond to zirconia so, different methods of surface treatment have been suggested to improve the adhesion of luting cements to oxide-based ceramic as: Micromechanical interlocking with airborne particle abrasion, physicochemical activation by silica-coated alumina particles ranging from 30 to 250 μm in size followed by silanization and chemical activation by cements containing functional monomer. [8] These monomers act as bifunctional molecules that connect with the surface oxide layer of metal based ceramic at one end and copolymerize with the resin cement matrix at the other end. [9]
10-methacryloyloxydecyl-dihydrogen-phosphate (10-MDP) is one of the most common type of these functional monomer. It was found that MDP monomers promote a water-resistant chemical bond to densely sintered zirconia ceramics. [10] Several studies reported that, the combination of both MDP primer and air-abrasion surface treatment has improved the bond strength of zirconia ceramic. [9]
Marginal adaptation of ceramic laminate veneers is the vertical distance between the finish line of the prepared tooth structure and the margins of the ceramic laminate veneers, [11] while internal adaptation is the perpendicular distance from the axial wall of the tooth structure and the fitting surface of the ceramic laminate veneer. [12] Adaptation of laminate veneer is measured by the intimate contact between the fitting surface of veneer and the prepared tooth structure. Composite resin cements are the weakest point in the porcelain veneer-resin cement-tooth complex so, intimate contact is recommended. [4] Any discrepancy in adaptation results in salivary infiltration, microleakage, dissolution of the luting cement, caries and pulpal damage. [13]
Marginal and internal adaptation of restorations can be measured by one of the following methods: Scanning electron microscope, optical microscope, transmission electron microscope, micro-computed tomography (micro-CT) and Silicone replica. [14] However, there is no standardized method to measure the fitness with absolute accuracy. [15]
Marginal and internal adaptation are considered a key criterion for evaluation of fixed restorations. High marginal and internal adaptation are recommended for long term clinical success, mechanical and biologic stabilization of the fixed prosthesis. [11] No previous studies have investigated the relation between different surface treatments and adaptation of zirconia ceramic restoration, so the aim of this in-vitro study was to evaluate the effect of different surface treatment materials on marginal and internal adaptation of zirconia ceramic laminate veneer.
The null hypothesis of this study was that, the different materials used for surface treatment didn’t have clear effect on marginal and internal adaptation of zirconia ceramic laminate veneer.
Materials and Methods
Preparation and replication of the abutments:
A maxillary central incisor ivory typodont tooth was selected to be the master abutment. An optical impression of the unprepared typodont tooth was taken using intraoral scanner (Omnicam Sirona, Germany) and saved as STL (Standard Tessellation Language) file to be used as a reference for fabrication of veneers with identical anatomy to the original typodont tooth. The resultant STL file was opened then the cutting tool of the CAD software (Ceramill Mind Ammann Girrbach, Germany) was used for removal of 2 mm from the incisal edge and the boundaries of the preparation were marked as the following: from labial surface; 0.5 mm away from the CEJ cervically, 1 mm beyond the mesio-buccal and disto-buccal line angles and from palatal surface; 1 mm from incisal edge with 0.5 mm palatal chamfer. [16] The marked areas were cut back with 0.55 mm uniform thickness. (Figure 1). The fiber reinforced composite blank (TRINIA, Bicon, U.S.A) was fixed in the milling machine holder (Ceramill Motion 2, 5-axis, Ammann Girrbach, Germany). Through the CAM software, milling order was sent to mill 28 identical prepared abutments with wet milling.

Figure 1: (A&B) Showing the design of the prepared typodont tooth in STL file (labially & palatally)
Abutment fixation:
To facilitate handling of the abutments during cementation, the root of each abutment was inserted vertically in transparent epoxy resin blocks by using a specially designed centralizing device (Figure 2).

Figure 2: Showing abutment fixation in epoxy resin block using centralizing device.
Fabrication of the zirconia laminate veneers:
The STL files of the prepared and unprepared typodont tooth were overlapped to each other using CAD software (Ceramill Mind Ammann Girrbach, Germany) to allow fabrication of the laminate veneers typical to the original typodont tooth outline and dimensions. By subtracting the two STL files, a new STL file of the laminate veneer was produced with a uniform thickness of 2.0 mm incisally and 0.5 mm facially and palatally. Fully stabilized zirconia blank (Ceramill Zolid fx, Amann Girrbach, Austria) was fixed in Ceramill Motion 2 milling machine holder to mill 28 identical laminate veneers with dry milling. The sprues were removed using zirconia cutting and finishing kit (EVE DIACERA, Germany). The veneers were then sintered in a ceramic furnace (Ceramill therm 3, Ammann Girrbach, Germany) according to the manufacturer's recommendations. The fitness of each veneer was checked to its corresponding abutment and all margins were evaluated using sharp dental explorer.
Surface treatment and specimens grouping of zirconia laminate veneers:: All zirconia laminate veneers were air abraded with 50 μm aluminum oxide particles at pressure 2 bar at 10 mm distance from the fitting surface for 10 seconds using sandblaster device (Renfert GmbH, Hilzingen, Germany) [15], cleaned in an ultrasonic cleaner containing distilled water for 5 minutes then dried with oil free compressed air. [17] The veneers were divided into four different groups (n=7) based on their surface treatment. Group A: treated with air abrasion only (control group). Group AZ: treated with air abrasion then conventional MDP-containing ceramic primer (Z-PrimeTM Plus, Bisco, U.S.A). Group AB: treated with air abrasion then universal ceramic primer (All-Bond Universal®, Bisco,U.S.A). Group AZB: treated with air abrasion, conventional ceramic primer (Z-PrimeTM Plus) and then universal ceramic primer (All-Bond Universal®).
Cementation of the veneers to the prepared abutments::
The prepared abutments were cleaned, etched by phosphoric acid 37% (Eco-Etch, Ivoclar Vivadent) for 15 sec. [4] then rinsed with air/water spray and gently dried by air flow then bonding agent (Tetric® N-Bond Universal, Ivoclar Vivadent) was applied and dried gently using air then light cured for 20 sec. using LED light-curing (Demi plus, Kerr). Adhesive cement (Variolink N LC, Ivoclar Vivadent) was applied to the fitting surface of each veneer then seated on its corresponding prepared abutment with light finger pressure for a few sec. then cured for 2-3 sec. The excess cement was removed carefully. Final light curing step was done for 40 sec. per surface starting from the palatal surface under constant static load of 250 g to ensure a uniform thickness of cement layer and standardize the applied load on all specimens during final polymerization. [3] (Figure 3)
Figure 3: Showing specimen cementation in a specially designed loading device.
Evaluation of marginal and internal adaptation:
After 24 hours distilled water storage at 37oC, [18] all specimens were sectioned at the center mesiodistally and incisogingivally perpendicular to the margins using Linear microsaw (IsoMet 4000, bluehler, Germany) resulted in 4 quadrants for each specimen. [4] The sectioned specimens were evaluated under stereo-microscope (Olympus SZ61, Tokyo, Japan) at 40X magnification combined with microscopic camera (TUCSEN, H Series China) and image processing software (T Capture 5.1, TUCSEN China). For each specimen, Absolute marginal gap (AMG) at cervical and incisal areas and internal gap (IG) at six different locations was measured: 1.0 mm away from the cervical margin, 1.0 mm away from the middle point toward the cervical, at the middle of the tooth incisogingivally (cervical quadrant), 1.0 mm away from the incisal margin, 1.0 mm away from the middle point toward the incisal and at the middle of the tooth incisogingivally (incisal quadrant). [4] (Figure 4)
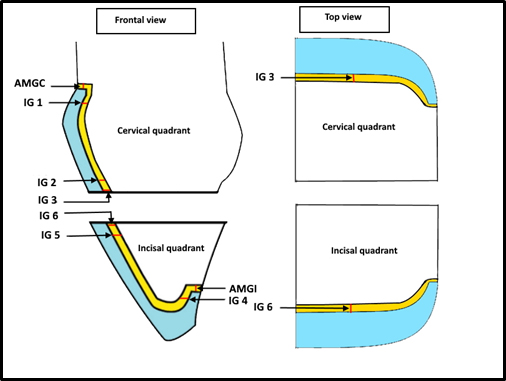
Figure 4: Showing schematic points of absolute marginal gaps and internal gaps measurements
AMGC: Absolute marginal gap cervically, AMGI: Absolute marginal gap incisally, IG 1: 1.0 mm away from the cervical margin, IG 2: 1.0 mm away from the middle point toward the cervical, IG 3: at the middle of the tooth incisogingivally (cervical quadrant), IG 4: 1.0 mm away from the incisal margin, IG 5: 1.0 mm away from the middle point toward the incisal and IG 6: at the middle of the tooth incisogingivally (incisal quadrant).
Statistical analysis
SPSS computer program version 23.0 was used to analyze the data. Descriptive data were presented in the form of Mean ± SD (Standard deviation). One-way ANOVA test was used to detect the significant difference between the four different groups of parametric data followed by post-hoc Tukey tests. P value <0.05 was considered statistically significant.
Results
The statistical analysis of AMG values of tested groups was showed in Table 1. One-way ANOVA test showed that, the mean AMG values were significantly lower in groups AZ, AB and AZB than the control Group A (p<0.001). Post-hoc Tukey test showed statistically significant differences between groups AZ, AB and AZB. The lowest AMG was recorded for Group AZ (95.93 ± 6.50 µm) followed by Group AZB (107.14 ± 7.42 µm) with significant difference P=0.01 between Group AZ and Group AZB.
| |
Group A |
Group AZ |
Group AB |
Group AZB |
P |
| Mean ±SD |
Mean ±SD |
Mean ±SD |
Mean ±SD |
| AMG |
151.07 ± 5.75 |
95.93 ± 6.50 |
127.50 ± 4.79 |
107.14 ± 7.42 |
< 0.001* |
| Post-hoc |
|
P1 =< 0.001* |
P1 =< 0.001*
P2 =< 0.001* |
P1 =< 0.001*
P2 =0.01*
P3 =< 0.001* |
|
Table 1: Showing statistical analysis of AMG values (µm) in the four tested groups
Data expressed as mean ±SD
SD: standard deviation P: Probability *: significance <0.05
Test used: One-way ANOVA followed by post-hoc Tukey
P1: significance vs Group A
P2: significance vs Group AZ
P3: significance vs Group AB
The statistical analysis of IG values of tested groups was showed in Table 2. One-way ANOVA test showed that the mean IG values were significantly lower in groups AZ, AB and AZB than the control Group A (p<0.001). Post-hoc Tukey test showed statistically significant difference between Group AZ and Group AB (p<0.001) and between Group AZ and Group AZB (p<0.001). The lowest IG was recorded for Group AZ (85.95 ± 4.39 µm) followed by Group AB and Group AZB (135.48 ± 5.22 µm and 140.48 ± 2.67 µm) respectively with no significant difference found between Group AB and Group AZB (P=0.17).
| |
Group A |
Group AZ |
Group AB |
Group AZB |
P |
| Mean ±SD |
Mean ±SD |
Mean ±SD |
Mean ±SD |
| IG |
167.62 ± 4.92 |
85.95 ± 4.39 |
135.48 ± 5.22 |
140.48 ± 2.67 |
< 0.001* |
| Post-hoc |
|
P1 =< 0.001* |
P1 =< 0.001*
P2 =< 0.001* |
P1 =< 0.001*
P2 =< 0.001*
P3 = 0.17* |
|
Table 2: Showing statistical analysis of IG values (µm) in the four tested groups
Discussion
The current in-vitro study was done to evaluate the effect of different surface treatment materials on marginal and internal adaptation of zirconia ceramic laminate veneer. Marginal and internal adaptation in this study was identified by the resin cement film thickness that reflected the real fit of the laminate veneer to its corresponding resin abutment.
The results of this in-vitro study showed that groups AZ, AB and AZB were significantly higher marginal and internal adaptation compared to Group A (control group), so the null hypothesis that different materials used for surface treatment didn’t have clear effect on marginal and internal adaptation of zirconia ceramic laminate veneer was rejected.
Standardized conditions were offered in this study to ensure accurate results, CAD/CAM TRINIA fiber reinforced composite abutments were chosen as they have modulus of elasticity (18.8 GPa) comparable to that of human dentin (11.59 to 27.30 GPa). [19] They also ensure uniform dimensions, homogenous composition and overcome the variations that may be found in natural teeth. [4] Upper central incisor was used as it is the most common tooth restored with a laminate veneer. [12]
Incisal overlap preparation design was performed to the abutment as incisal coverage with ceramic veneers has been suggested to enhance the survival rate of the restoration, esthetics of incisal edge and better seating of the veneer. It also provides a stronger bulk of ceramic resulting in decreasing of crack lines and fractures occurrence on the palatal side. [20]
For standardization of abutments preparation, Ammann Girrbach CAD/CAM system was used for designing and milling of the abutments to avoid human mistakes that can occur during manual preparation. [11]
All laminate veneers were fabricated using CAD/CAM system with no internal adjustment as this achieves an industrial standard than prostheses produced manually. [21] Die spacer was digitally adjusted with 50 μm for all veneers in this study as it was previously stated by studies that the fit of restoration margins are greatly affected by adequate die spacing. [11]
In this study, Zolid fx laminate veneers were used as it is a high translucent zirconia ceramic that have been recently introduced. It indicated for several clinical conditions and gives esthetically desirable outcomes with discolored teeth,15 besides its excellent optical properties, high compatibility and superior mechanical properties than other glass based ceramic. [22]
Air abrasion used in the present study was done by 50 µm Al2O3 particles at pressure 2 bar to avoid surface damage. [9] Air abrasion is the most preferred method for zirconia ceramics surface roughening as it increases the wettability and the surface energy but creates micro-cracks on the zirconia surface. However, resin luting flaws into these microcracks and strengthen the ceramic, [23] so it was used as a control group.
Variolink N conventional resin cement was selected in this study for cementation of zirconia laminate veneers as it has no MDP monomer and used as a control to compare the effect of different MDP containing materials in surface treatment. [9]
In this study marginal and internal adaptation were measured after cementation by sectioning of the veneers mesiodisally and incisogingivally, so internal gaps can be visualized easily at any part of the tooth desired. [11] However marginal adaptation measurements are limited to distinct points. [15]
In the present study the highest marginal adaptation was recorded for Group AZ with AMG 95.93 ± 6.50 µm followed by Group AZB with AMG 107.14 ± 7.42 µm, while Group A recorded the lowest marginal adaptation with AMG 151.07 ± 5.75 µm. For internal adaptation, Group AZ recorded the highest internal adaptation with IG 85.95 ± 4.39 µm followed by Group AB and Group AZB with IG 135.48 ± 5.22 µm and 140.48 ± 2.67 µm respectively, while Group A recorded the lowest internal adaptation with IG 167.62 ± 4.92µm.
To our knowledge, there is no previous studies compared the effect of Z-Prime Plus and All-Bond Universal on marginal and internal adaptation of zirconia ceramic, however the results of this study can be partially supported with a study done by Sharafeddin and Shoale, (2018) [9] in which they found that, zirconia surface treatment with application of Z-Prime Plus after air abrasion has significant higher shear bond strength values (22.45 ± 3.60 MPa) than All-Bond Universal application after air abrasion (17.51 ± 1.34 MPa) and air abrasion control group recorded the lowest shear bond strength values (7.58 ± 1.62 MPa). They referred the higher bond strength for both Z-Prime Plus and All-Bond Universal to the presence of MDP monomer in their composition which enhances the chemical affinity of zirconia. MDP is an amphiphilic structure which has hydrophobic vinyl group end that can copolymerize with the resin monomer and hydrophilic phosphate group end that can react with the hydroxyl groups on the zirconia surface, however the highest bond strength was recorded for Z-Prime Plus as a result of the synergistic effect between acidic MDP and carboxylic monomer in its composition.
In addition to the previously mentioned explanations, Z-Prime Plus forms a thin film when compared with All-Bond Universal [18] so, it showed the highest marginal and internal adaptation in our study.
The results of the present study was also in agreement with the research work of Shehata et al. (2018) [17] as they found that zirconia surface treatment by sandblasting with 110 µm Al2O3 particles and application of Z-Prime Plus recorded significant higher shear bond strength (10.007 ± 2.9 MPa) than sandblasting without primer application (5.1232 ± 0.435 MPa). Similarly, Tanis et al. (2015) [23] found that MDP containing priming agent (Z-Prime Plus) after air abrasion with 50 µm Al2O3 particles significantly increased the bond strength of zirconia with resin cement (15.25 ± 1.20 MPa) than air abrasion only (11.34 ± 2.07 MPa).
The results of the current study were disagreed with Omidi et al. (2018) [24] as they found that application of Universal Adhesive to sandblasted zirconia blocks with 50 µm Al2O3 particles showed higher bond strength (25.70 ± 2.01 MPa) than Z-Prime Plus primer application to the sandblasted blocks (19.16 ± 3.53 MPa). This difference may be related the artificial aging they performed (2500 thermal cycles) to all samples.
This study was the first study to evaluate the combination effect of Z-Prime Plus and All-Bond Universal application after air abrasion (Group AZB) surface treatment on adaptation of zirconia laminate veneer. The aim of this combination was to evaluate the effect of increased MDP concentration with presence of carboxylic monomer on the adaptation of zirconia veneers. The results showed that, this group has lower marginal and internal adaptation than Group AZ, so increased MDP concentration didn’t improve the marginal and internal adaptation. However, when comparing Group AZB with Group AB, Group AZB showed better marginal adaptation this may be related to the presence of carboxylic monomer in its composition, but there is no significant difference in internal adaptation between them, this may be related to the thick film formed during polymerization of All-Bond Universal in both groups. [18]
dos Santos et al. (2019) [18] found no significant difference in bond strength between the combination of Z-Prime Plus and All-Bond Universal group, Z-Prime Plus group and All-Bond Universal group when they were applied on sandblasted zirconia blocks with 50 µm Al2O3.
All tested groups except air abrasion control group (Group A) showed acceptable clinical performance. However, the clinical significant of present study supported the choice of Z-Prime Plus after air abrasion (Group AZ) for zirconia surface treatment as it recorded the highest marginal and internal adaptation of zirconia laminate veneer besides its simple clinical application as it doesn’t require light cure that is beneficial when compared to the universal adhesive systems.
This study has some limitations including: small sample size and no artificial aging was performed to assess the longevity of this study as it was reported by previous studies that marginal and internal integrity are affected by occlusal stresses, thermocycling and dynamic loading which lead to microleakage that caused by the hydrolytic effect of resin-based luting agents. [15] Thus it is recommended to perform further assessment of different surface treatment on marginal and internal adaptation of zirconia laminate veneer after artificial aging.
Conclusion
Under the limitations of this in-vitro study, the following conclusions could be obtained:
- Different materials used for surface treatment affected the marginal and internal adaptation of zirconia ceramic laminate veneer.
- Both mechanical and chemical surface treatments were recommended for improving the marginal and internal adaptation of zirconia ceramic laminate veneer.
- Surface treatment using air abrasion then Z-Prime Plus effectively improved the marginal and internal adaptation of zirconia ceramic laminate veneer.
References
- Asra Sabir Hussain. “Esthetic Restorative Treatment Planning for Dental Professionals: An Overview”. EC Dental Science 15.5 (2017): 191-195.
- Garcia-Baeza D., et al. “Soft and hard tissue management in the treatment of a discolored single tooth in the esthetic zone”. International Journal of Esthetic Dentistry 12.1 (2017): 28-40.
- Hamza TA., et al. “Effect of artificially accelerated aging on margin fit and color stability of laminate veneers”. Stomatological Disease and Science 2.1 (2018): 1-7.
- Al-Dwairi ZN., et al. “A comparison of the marginal and internal fit of porcelain laminate veneers fabricated by pressing and CAD-CAM milling and cemented with 2 different resin cements”. Journal of Prosthetic Dentistry 121.3 (2019): 470-476.
- Sadighpour L., et al. “Fracture resistance of ceramic laminate veneers bonded to teeth with class v composite fillings after cyclic loading”. International Journal of Dentistry (2018).
- Subaşi MG and Inan Ö. “Influence of surface treatments and resin cement selection on bonding to zirconia”. Lasers in Medical Science 29.1 (2014): 19-27.
- Prado M., et al. “Ceramic surface treatment with a single-component primer: Resin adhesion to glass ceramics”. The Journal of Adhesive Dentistry 20.2 (2018): 99-105.
- Rebholz-Zaribaf N and Ozcan M. Adhesion to zirconia as a function of primers/silane coupling agents, luting cement types, aging and test methods. Journal of Adhesion Science and Technology 31.13 (2017): 1408-1421.
- Sharafeddin F and Shoale S. “Effects of universal and conventional MDP primers on the shear bond strength of zirconia ceramic and nanofilled composite resin”. Journal of Dentistry 19.1 (2018): 48-56.
- Grasel R, Santos MJ., et al. “Effect of resin luting systems and alumina particle air abrasion on bond strength to zirconia”. Operative Dentistry 43.3: 282-290.
- Tammam R. “Investigation the effect of restorations fabricated with CAD / CAM technology, the heat-press technique and type of resin cement on marginal and internal adaptation of all ceramic crowns”. Advances in Dentistry & Oral Health 5.2 (2017): 1-13.
- Fadhil NH., et al. “Evaluation of marginal and internal adaptation of CAD / CAM and pressable ceramic veneers of different preparation designs using silicone replica technique : A comparative in vitro study”. International Journal of Science and Research 6.8 (2017): 2222–2227.
- Ranganathan H., et al. “Cervical and incisal marginal discrepancy in ceramic laminate veneering materials: A SEM analysis”. Contemporary Clinical Dentistry 8.2 (2017): 272-278.
- Yuce M., et al. “Comparison of marginal and internal adaptation of heat-pressed and CAD/CAM porcelain laminate veneers and a 2-year follow-up”. Journal of Prosthodontics 28.5 (2019): 504-510.
- Kusaba K., et al. “Effect of preparation design on marginal and internal adaptation of translucent zirconia laminate veneers”. European Journal of Oral Sciences 126.6 (2018): 507-511.
- Arora A., et al. “Evaluation of fracture resistance of ceramic veneers with different preparation designs and loading conditions: An in vitro study”. The Journal of Indian Prosthodontic Society 17.4 (2017): 325-331.
- Shehata WK., et al. “Effect of sandblasting and zirconia primer application on the zirconia-cement shear bond strength (An in-vitro study)”. AL-AZHAR Dental Journal 5.2 (2018): 187-194.
- Ricardo Alves dos Santos., et al. “Can universal adhesive systems bond to zirconia?”. Journal of Esthetic and Restorative Dentistry 31.6 (2019).
- Aldafeeri HR., et al. “Marginal accuracy of machinable monolithic zirconia laminate veneers”. IOSR Journal of Dental and Medical Sciences 18.5 (2019): 67-74.
- Albanesi RB., et al. “Incisal coverage or not in ceramic laminate veneers : A systematic review and meta-analysis”. Journal of Dentistry 52 (2016): 1-7.
- Banour F. “Marginal accuracy of minimal and no-preparation of two different machinable ceramic laminate veneers”. Master thesis, Mansoura University, Mansoura, Egypt. 2017.
- Blatz MB., et al. “The effect of resin bonding on long-term success of high-strength ceramics”. Journal of Dental Research 97.2 (2018): 132-139.
- Tanış MÇ., et al. “Resin cementation of zirconia ceramics with different bonding agents”. Biotechnology & Biotechnological Equipment 29.2 (2015): 363-367.
- Omidi BR., et al. “Comparison of micro-shear bond strength of treatments using universal adhesive and zirconia”. Journal of Lasers in Medical Sciences 9.3 (2018): 200-206.
Citation:
Mohamed Hamed Ghazy., et al. “Influence of Different Types of Surface Treatment on Adaptation of Ceramic Laminate Veneer”. Oral Health and Dentistry 4.1 (2020): 16-24.
Copyright: © 2019 Mohamed Hamed Ghazy., et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
































;)
;)
;)
;)
 Scientia Ricerca is licensed and content of this site is available under a Creative Commons Attribution 4.0 International License.
Scientia Ricerca is licensed and content of this site is available under a Creative Commons Attribution 4.0 International License.